In response to daunting provider workforce challenges, states are passing hospital staffing laws intended to increase patient safety and reduce nurse burnout. As of February 2024, 15 states have passed acts regarding hospital nurse staffing, and a handful of other states are in the process of considering similar bills.i
This state-level activity has also prompted policy discussions and introduction of the Nurse Staffing Standards for Hospital Patient Safety and Quality Care Act of 2023, which would be the first federal law to address nurse staffing if passed.
Why it matters:
Existing and proposed requirements
Nurses have been discussing staffing standards for decades. Many feel overwhelmed with their workloads and worry that existing staffing levels do not always allow for safe patient care. High turnover rates and the loss of experienced nurses put a higher burden on the remaining experienced nurses, who have a greater workload and must train travel nurses and/or new nurses. In addition, many feel their contributions are minimized by hospital administrators and patients, despite their significant efforts to provide high-quality care while also feeling under-resourced. Given these dynamics, nursing associations, state legislatures, and other healthcare advocacy organizations have been advancing this topic.
The specifics of state laws and mandates vary, though most fall into 1 or more of these 3 categories:
- Legally mandated nurse-to-patient ratios: While California established mandated nurse-to-patient ratios more than 20 years ago, only 2 other states have followed suit: Massachusetts and Oregon. The ratios vary by type of unit (e.g., ICU, general Medical/Surgical, Psychiatric). In some cases, as in Massachusetts, the ratio in the ICU is adjusted depending on the stability of the patient.
- Required staffing committees: Nine states (Connecticut, Illinois, Minnesota, New York, Nevada, Ohio, Oregon, Texas, and Washington) require hospital-based staffing committees composed of a minimum of 50% direct care nurses. In some cases, committees must have at least 1 more nurse than the total of other represented professionals on the committee for voting purposes. Some states (e.g., Connecticut) stipulate that collective bargaining entities are entitled to pick the nurse committee members.
- Disclosure/reporting requirements: Five states (Illinois, New Jersey, New York, Rhode Island, and Vermont) require an annual or biannual submission of staffing plans. Plan requirements can include elements such as staffing ratios by type of clinician on each unit and/or by patient acuity level, data/input considered when establishing ratios, implementation and oversight process, quality measures, and more. Some states also require regular reporting on staffing plan compliance and any actions taken to resolve variances compared to the standards.
Established nurse-to-patient ratios are more widespread than the states with laws in place. Although only 3 states—California, Massachusetts (ICU only), and Oregon—have mandated ratios, hospitals throughout the U.S. have adopted similar practice standards.
On the federal side, the Nurse Staffing Standards bill proposes tailored minimum direct care nurse-to-patient ratios for the following units: trauma ER, operating rooms, critical care, emergency department, step down, medical/surgical, acute care psychiatry, intermediate care nursery, inpatient rehabilitation, post-partum, and well-baby. The bill also would require staffing committees to be responsible for developing and implementing the organization’s staffing plan, which would need to comply with the stated minimum nurse-to-patient ratios. The committee must have “at least one registered nurse from each hospital unit and shall be composed of at least 50% direct care registered nurses.” ii
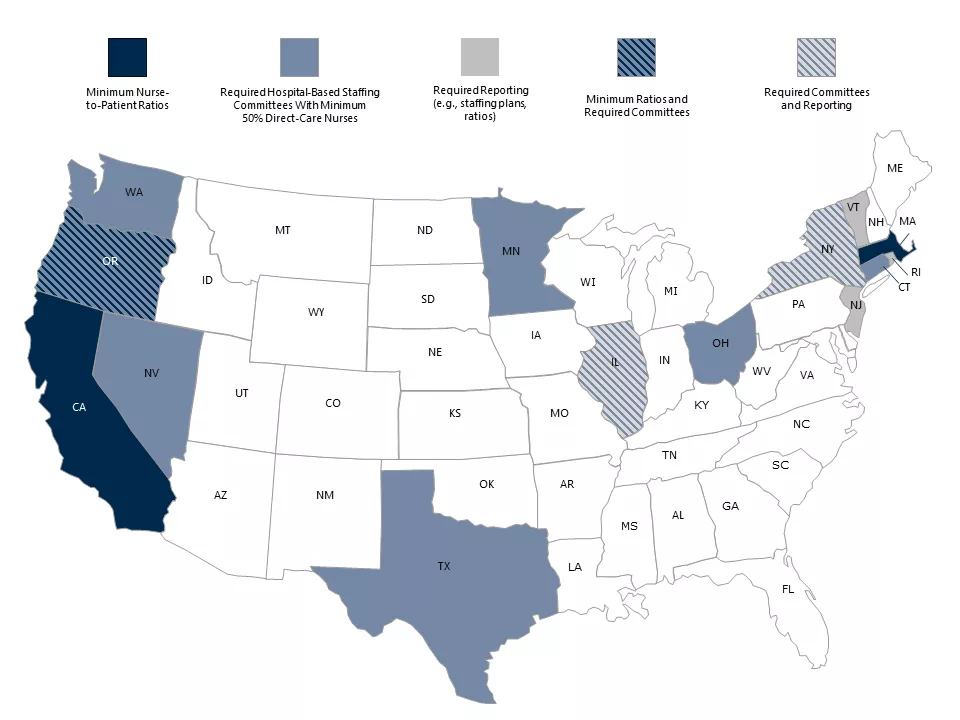
Figure sources: (1) Alexa Davidson, “Nurse-to-Patient Staffing Ratio Laws and Regulations by State,” Nurse Journal, March 21, 2023, https://nursejournal.org/articles/nurse-to-patient-staffing-ratio-laws-by-state/. (2) Washington State Nurses Association, “New Oregon Law Establishes Safe Staffing Ratios,” The Washington Nurse, October 20, 2023, https://www.wsna.org/news/2023/new-oregon-law-establishes-safe-staffing-ratios.
The major issue that remains unaddressed
Minimum staffing ratios are intended to support safe patient care and a healthier workforce, shared objectives of both organization leaders and front-line workers. Although these requirements can achieve some of these objectives, they don’t solve the supply-demand imbalance: the pervasive, persistent shortage of nurses that is unlikely to abate in the near or distant future.
This imbalance of nursing supply and patient demand is driven in part by a lack of nurse educators (creating a bottleneck in the pipeline), early retirement (largely due to burnout), and an increasing number of established nurses taking on more flexible hours and/or administrative roles, among other factors.
What’s next:
Hospitals must navigate through these complex dynamics, developing a planning process that can produce a staffing model that is safe, fair, and achievable. Hospital administrators should view their staffing committee as a partner, working together toward a common goal. Critical factors include:
-
Equip committee members with an understanding of all facets of the planning process. The staffing planning process is much more than setting nurse-to-patient ratios and trying to implement them. Committee members need to become familiar with the inputs and analytics involved, such as the variety of current and emerging staffing models across the country, the economics (including staff expense vs. patient revenue, recruitment costs, and more), and any mandates or rules set by the state or organized labor groups.
-
Facilitate first-hand knowledge of each department’s needs and drivers of burnout. Committee members should spend time in all departments to gain a comprehensive understanding of the current staffing in each—not only nurses but the entire care team and support staff, such as lab and transport. They should get to know the process by which departments determine and schedule staff, key issues and pain points that may be unique to that department or unit, drivers of burnout,iii and best practices that could be adopted in other areas of the hospital.
While nursing staffing is the focus of state laws, it will be important to take a similarly thoughtful approach to planning for other groups of hospital staff, including critical technical staff in areas such as sterile processing and nonclinical employees, such as food service and environmental staff. -
Empower the committee to bring forth innovative ideas around care models and new processes and procedures. Allow the group time and resources to support the exploration of new care models that would alleviate the stress experienced by many front-line colleagues. Care model and technology innovations can create more efficient use of nurses’ time and greater satisfaction with the activities for which they are responsible.
Examples of new models could include incorporating unlicensed personnel into care teams or integrating other professionals into the care team. That would change the skill mix of the team and could move appropriate tasks away from nurses—focusing nurses on specific interventions and the care only they can deliver. This could translate into more total staff hours but at a more cost-effective rate. Similarly, technologies that reduce nurses’ administrative task loads and/or make care more efficient could potentially reduce the total number of staff required. -
Entrust the committee with making progress. The group should be responsible for tracking and reporting staffing data, outcomes, feedback, challenges, and successes. And organization leaders should recognize the committee for its accomplishments and achievements.
The following questions can help hospital executives get started or extend existing workforce planning efforts in a more productive way:
-
How are we balancing efforts to comply with state laws while also advancing how we approach patient care?
-
What processes do we have to understand the daily experience of front-line staff at an actionable level of detail (including burnout impact and trends over time)?
-
How are we encouraging innovation that would lead to new care models?
-
How will we define success, and how will we measure and report progress?
-
How are we advocating for what we believe are appropriate and effective state and national laws around hospital staffing?
The nurse staffing shortage is unlikely to significantly abate anytime soon. While mandated or negotiated staffing ratios do not address that problem, they are a reality for many organizations. Hospitals should take a planful, strategic approach to staffing. This approach should include empowering their staffing committees to identify opportunities to optimize the planning process and implement innovative solutions. The ultimate goal is ensuring a professionally satisfied, engaged workforce that is well-equipped to provide excellent patient care.


